What it is
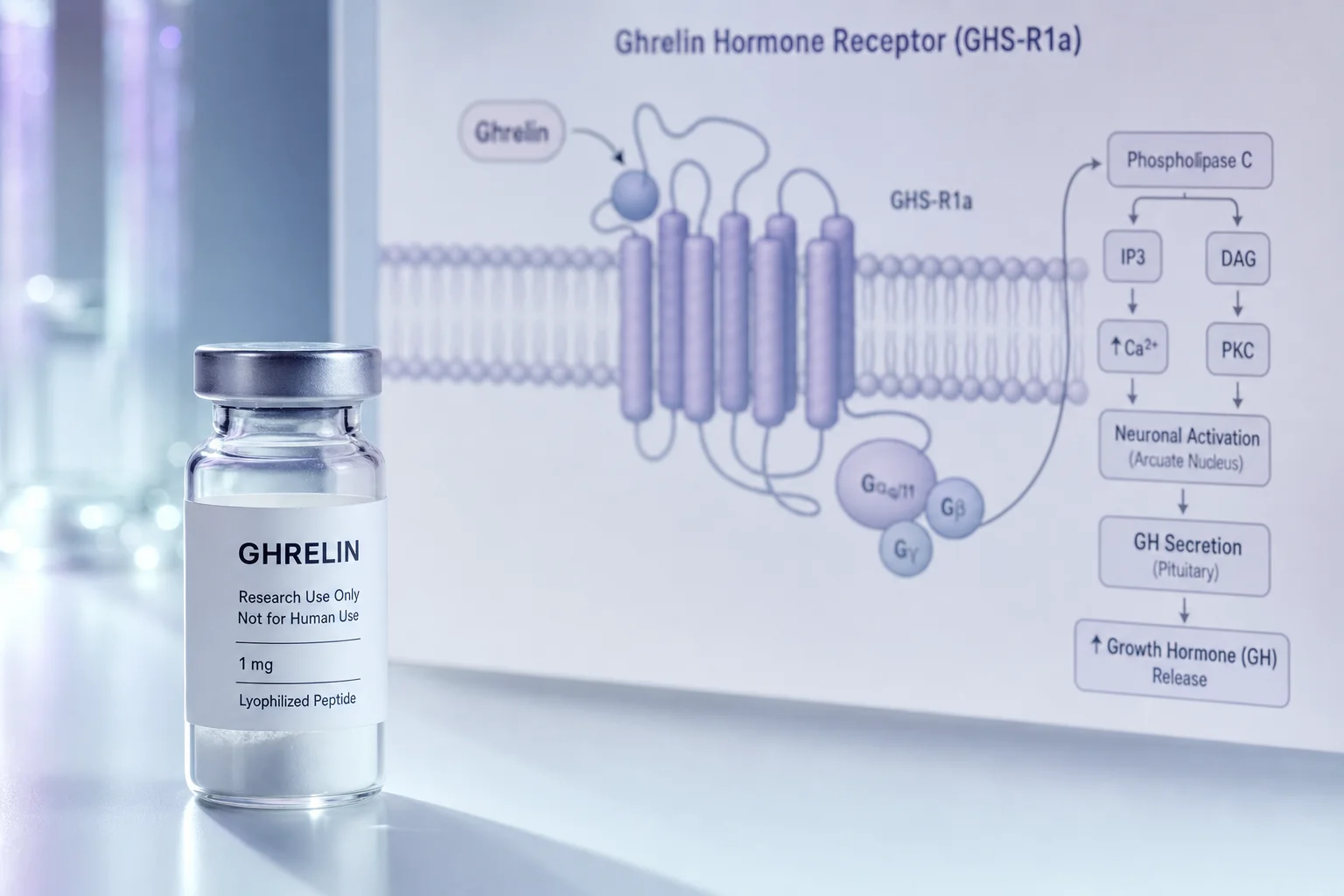
GHRP-2 (growth hormone-releasing peptide 2), also known by the pharmaceutical name pralmorelin, is a synthetic hexapeptide that acts as an agonist at the ghrelin receptor (GHSR-1a) in the pituitary and hypothalamus. Like endogenous ghrelin, binding at this receptor triggers growth hormone secretion, though GHRP-2 is a purely synthetic compound with no structural relation to ghrelin itself.[1]
GHRP-2 was developed by researchers at Tulane University as part of a series of synthetic GH secretagogues that also includes GHRP-6 and Hexarelin. It is approved in Japan as Pralmorelin (KP-102) for diagnostic testing of GH deficiency and hypothalamic-pituitary function; it is not FDA-approved in the United States. Unlike ipamorelin, GHRP-2 produces concurrent elevations in cortisol and ACTH alongside GH release.
What researchers study it for
- Growth hormone secretion stimulation Ghigo et al. reviewed GHRP-2 as one of several synthetic GHRPs that produce marked, dose-related GH release in humans after intravenous, subcutaneous, intranasal, and oral administration, with effects acting through ghrelin receptors at both pituitary and hypothalamic levels.[1]
- Diagnostic testing for GH deficiency The GHRP-2 stimulation test is used clinically in Japan for diagnosing GH deficiency; Suzuki et al. evaluated its clinical utility in patients with hypothalamic-pituitary disorders, finding it provided useful information for diagnosing GHD and concurrent adrenal insufficiency due to its stimulation of both GH and ACTH pathways.[5]
- GH stimulation in pediatric populations The GHRP-2 loading test is referenced in pediatric endocrinology for provocative GH testing; a retrospective study of adolescents found robust GH peak responses in those without organic GHD, supporting its established cut-off thresholds for identifying true GH deficiency.[2]
- Appetite stimulation and ghrelin pathway research In a human crossover study, Laferrère et al. found that subcutaneous GHRP-2 infusion increased ad libitum food intake by approximately 36% compared with saline, with every participant eating more; the researchers proposed GHRP-2 as a useful tool for investigating ghrelin's role in eating behavior without the variable pharmacokinetics of native ghrelin.[3]
- Lean body mass and wasting states Sigalos and Pastuszak reviewed GH secretagogue literature, noting preclinical and early clinical evidence suggesting GHRPs including GHRP-2 may improve lean mass in wasting conditions, reduce fat mass, and enhance exercise capacity through pulsatile GH stimulation, though long-term rigorous trials remain limited.[4]
- GH axis feedback preservation A key area of research interest in GHRPs is that they stimulate endogenous GH release through intact pituitary pathways rather than replacing GH directly; this means GH production remains subject to natural feedback mechanisms, which researchers have proposed as a safety advantage over exogenous GH administration.[4]
Research context
GHRP-2 has been under investigation since the 1990s and has one of the more established clinical profiles among synthetic GHRPs, partly because it received pharmaceutical approval in Japan as a diagnostic agent. The diagnostic application is well-characterized: standardized GHRP-2 stimulation testing is used clinically in Japan, with established cut-off thresholds for GH peak responses that differentiate GH-deficient from healthy subjects.[5] The compound is consistently among the most potent GH secretagogues studied in humans, producing GH increases that are generally larger than those seen with GHRP-6 at equivalent doses, though this also means more pronounced cortisol and ACTH co-stimulation.[1]
Research on therapeutic applications (body composition, anti-aging, wasting states) is less well-controlled. Most studies examining these outcomes have been short-term, involved small samples, or were conducted as retrospective reviews rather than randomized trials.[4] The appetite-stimulating effect documented in the Laferrère et al. human study adds an important dimension: GHRP-2 acts on ghrelin receptors broadly, and its appetite-stimulating activity is not a side effect that can easily be dissociated from its GH-stimulating effects.[3] Researchers working with this compound in body composition contexts should account for this as a confounding variable.
Typical research parameters
| Parameter | Detail |
|---|---|
| Common vial sizes | 2 mg, 5 mg (10 mg available from some research vendors) |
| Supplied as | Lyophilized powder; reconstituted with bacteriostatic water before use |
| Storage | Refrigerate; lyophilized powder stable at room temperature short-term; protect from light and heat |
| Stability | Lyophilized: 24+ months under appropriate conditions; reconstituted: approximately 28 days refrigerated |
| Administration studied | Subcutaneous injection (primary research and diagnostic use); intravenous (diagnostic stimulation testing); intranasal and oral routes explored in early pharmacokinetic work |
References
- [1] Ghigo E, Arvat E, et al. Growth hormone-releasing peptides. Eur J Endocrinol. 1997;136(5):445-60. PubMed ↗
- [2] Onuki T, Hiroaki T, et al. Robust growth hormone responses to GH-releasing peptide 2 in adolescents. J Pediatr Endocrinol Metab. 2024;37(8):730-733. PubMed ↗
- [3] Laferrère B, Abraham C, et al. Growth hormone releasing peptide-2 (GHRP-2), like ghrelin, increases food intake in healthy men. J Clin Endocrinol Metab. 2005;90(2):611-4. PubMed ↗
- [4] Sigalos JT, Pastuszak AW. The Safety and Efficacy of Growth Hormone Secretagogues. Sex Med Rev. 2018;6(1):45-53. PubMed ↗
- [5] Suzuki S, Ruike Y, et al. Clinical Usefulness of the Growth Hormone-Releasing Peptide-2 Test for Hypothalamic-Pituitary Disorder. J Endocr Soc. 2022;6(8):bvac088. PubMed ↗