
Some peptides are available by prescription. Others are sold with labels that say "for research use only." That distinction isn't just legal fine print. It reflects something real about what we know, how confident we are, and who has reviewed the evidence behind a compound.
What FDA approval actually means
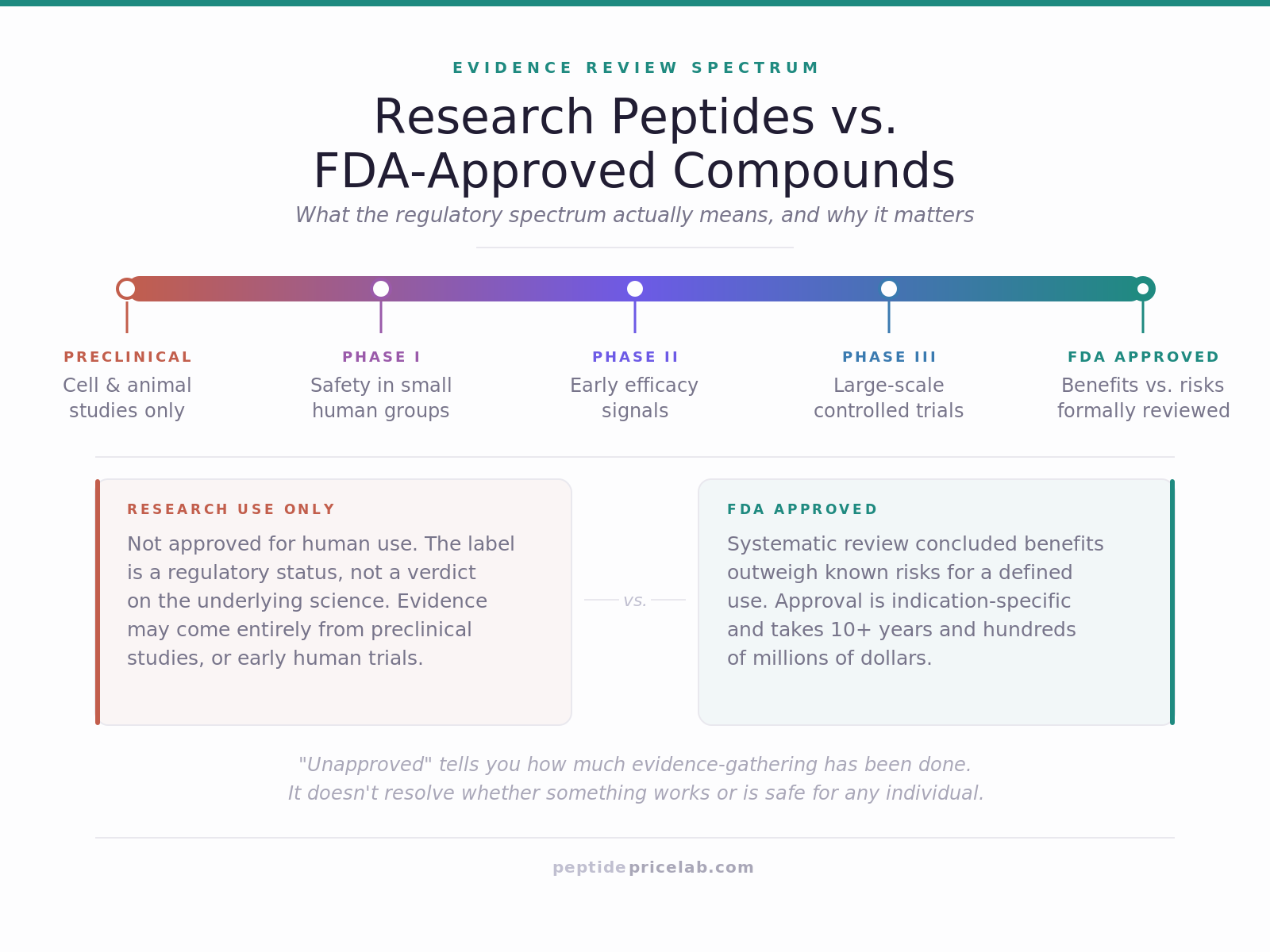
The FDA (the U.S. Food and Drug Administration) approves drugs for specific uses after a structured evidence-gathering process. Here's roughly how that works:
- Preclinical research: The compound is tested in cells and animals. This generates early data on how it behaves, what doses do what, and whether obvious harms show up. Most compounds that enter this phase never make it further.
- Phase 1 trials: A small group of human participants (often healthy volunteers) receive the drug primarily to assess safety. Researchers are watching for adverse effects and figuring out how the body processes the compound.
- Phase 2 trials: A larger group, usually people with the condition the drug is meant to address, receive the compound. Researchers are now looking for signs that it works, while continuing to monitor safety.
- Phase 3 trials: Larger still. Often thousands of participants, often compared against a placebo or existing standard of care. This is where you get the data that supports or undermines the efficacy claim.
- FDA review: The agency reviews the submitted data, often consulting independent advisory panels. If the benefit-risk profile meets their standard, the drug is approved for the specific indication it was tested for.
The whole process typically takes over a decade and costs hundreds of millions of dollars. The FDA approval doesn't mean a drug is perfect or without risk. It means a systematic review concluded the benefits outweigh the known risks for a defined population and use case.
Importantly, approval is indication-specific. Semaglutide (sold as Ozempic and Wegovy) is approved for type 2 diabetes and weight management. It is not FDA-approved for every possible use case someone might theorize for it.
What "research use only" means
A compound sold as "for research use only" (sometimes written as "not for human use") has not been through FDA approval. In the United States, that means it cannot legally be sold as a drug, marketed for human consumption, or prescribed. The label is both a legal designation and a description of where the compound sits in the development pipeline.
In practice, most research peptides are sold by chemical suppliers to laboratories for use in cell studies, animal models, and early-stage investigations. That's a legitimate and important part of how science works. A compound has to be studied before it can be approved.
What the label does not tell you is whether the compound is promising, dangerous, or somewhere in between. "Not FDA-approved" is a regulatory status, not a verdict on the science. A compound can be unapproved because it hasn't been studied in humans yet. It can also be unapproved because it was studied and failed. The label doesn't distinguish between those situations.
The spectrum from approved to preclinical
It helps to think of this not as a binary but as a spectrum.
At one end: fully approved compounds like insulin (approved since 1982 in recombinant form), oxytocin, and semaglutide. These have well-established safety and efficacy data for their approved uses. They're prescribed by licensed clinicians and dispensed by pharmacies.
A step down: compounds that are approved for some uses but studied for others. Bremelanotide, for example, is FDA-approved for hypoactive sexual desire disorder in premenopausal women. But it's also studied for other applications where it doesn't have approval. In those unapproved applications, it carries the same uncertainty as any research compound.
Further along the spectrum: compounds currently in clinical trials. These have cleared preclinical hurdles and are being tested in humans under controlled conditions, but approval (if it comes) is years away. The evidence base is real but incomplete.
At the other end: compounds that are preclinical only, meaning the evidence comes entirely from cell cultures and animal models. The mechanisms may be interesting. The animal data may be promising. But we don't yet know how that translates to humans, and it often doesn't translate the way early research suggests.
Where compounding pharmacies fit in
A compounding pharmacy is a licensed pharmacy that prepares customized medications, often to meet a patient's specific needs that off-the-shelf drugs can't address. They operate under FDA oversight (via Section 503A and 503B of the Federal Food, Drug, and Cosmetic Act) and can legally produce certain compounds, including some peptides, for patients with a valid prescription.
This is how some peptides without full FDA approval can still reach patients through legitimate medical channels. A physician prescribes, a licensed compounding pharmacy prepares the compound, and the patient fills the prescription. It's a legal pathway, but quality control varies by pharmacy, and the compound still doesn't carry the full evidence base of an FDA-approved drug.
Unapproved doesn't mean ineffective, or safe
Approval status and effectiveness are related but separate questions. A compound can be unapproved and show a strong signal in animal models. That's a real finding. It's also not the same as knowing it works safely in humans at specific doses. The history of drug development includes many compounds that looked excellent in animals and performed poorly or caused harm in human trials.
Conversely, every approved drug has side effects, contraindications, and patient populations for whom it's not appropriate. The difference is that for approved drugs, those risks have been characterized systematically, and prescribing clinicians have access to that data. Approval status tells you how much evidence-gathering has been done, and who has reviewed it. It doesn't automatically resolve whether something works or is safe for any individual.
Questions worth asking before engaging with a research compound
These are the questions that separate informed engagement from guesswork:
- Where does the evidence come from? Animal studies only, or human trials? If human trials, what phase and how large?
- What were the outcomes measured? Surrogate markers (a change in a blood value) are not the same as clinical endpoints (reduced incidence of disease).
- Who is the supplier and what quality controls do they use? For research peptides, purity and accurate concentration matter. Third-party testing certificates are a baseline standard.
- Is there a qualified clinician involved? If you're considering any actual use, a physician who understands the evidence base is the right starting point, not a forum or a vendor.
- What does the risk profile look like? Not just "is it approved" but what adverse effects have been reported, and in what contexts?
Where to go from here
If you're curious about a specific compound and where it sits on this spectrum, the Research Notes section covers individual peptides in detail, including a summary of the evidence, typical study parameters, and current pricing data.
If you're newer to what peptides are in the first place, the guide What Are Peptides, Really? covers the biological basics first.